On June 18, GPNi hosted a special live webinar and podcast recording on site at the ISSN 2026 Annual Conference. The topic was simple on the surface, but much more complex once the discussion began: peptides.
The level of interest around the session said a lot about where this topic is heading. Nearly 120 people registered in advance, joining from countries including the United States, Canada, Brazil, Chile, the United Kingdom, Germany, China, and Japan. The audience included sports nutritionists, registered dietitians, athletes, coaches, students in sports nutrition, business owners, and professionals working across the nutrition and health industries.
More than 70 attendees joined the live session. Because the webinar served a global audience, time zones and work schedules made live attendance difficult for some registrants. Many who could not attend live reached out afterward to ask about the replay.
GPNi is now preparing the full replay and selected highlight clips. Subtitles will also be added to make the content easier to follow for international audiences. At the beginning of the live session, the GPNi team also walked attendees through Zoom’s AI caption and translation features, helping non-native English speakers follow the discussion more comfortably.
Still, the most important part of the event was not the turnout. It was the conversation itself.

This Was Not a Peptide Promotion Session
GPNi Founder and CEO Drew Campbell made the tone clear from the start. This webinar was not designed to promote peptide products. It was not about telling people what to use, where to buy it, or how to take it.
Instead, the goal was to clarify what peptides are, which ones are approved, which ones are still being studied, and how dietitians, coaches, athletes, and consumers should think about the boundaries around them.
Over the past few decades, sports nutrition has seen plenty of major trends, from creatine to CBD. But peptides feel different. They are no longer just being discussed in gyms or among high-performance athletes. They have moved into weight management, medical clinics, wellness spaces, households, and social media.
That is exactly why the conversation needs more clarity.
Rick Collins: Start by Understanding the Category
One of the featured guests was Rick Collins, whom Drew introduced as the “Peptide Lawyer.” The title fits. Rick has spent years working at the intersection of health, fitness, dietary supplements, and regulation. So his part of the discussion did not begin with “what works.” It began with law, regulation, and product identity.
Rick first explained that peptides are short chains of amino acids. Insulin is a peptide. Growth hormone is a peptide. Collagen-related products may also be described using peptide language. In nutrition, hydrolyzed proteins and collagen peptides are familiar examples.
But that does not mean all peptides belong in the same category. It also does not mean they are regulated in the same way.
That was one of Rick’s main points throughout the webinar. Just because something is called a peptide does not automatically make it a supplement, a natural amino acid product, or something that can be treated casually.
On social media, peptides are often described in overly simple terms. You may hear someone say, “It’s just amino acids.” But that can be misleading. Many drug-like peptides are made from amino acids, but they are specifically designed or modified to create stronger, longer-lasting, or more targeted effects in the body. They are not the same thing as protein powder or a basic amino acid supplement.
From a regulatory standpoint, Rick outlined three broad categories.
The first category includes peptides that are already approved prescription drugs, such as GLP-1-related medications. These products should be used under medical supervision.
The second category includes newer compounds that are still in development or moving through the approval process. Retatrutide was one example discussed during the webinar. It may represent a future direction in weight management, but it should not be treated as if it were already a fully approved, mature medication. That is where risk begins to enter the conversation. The complete safety and efficacy data have not yet gone through the full approval process.
The third and more complicated category includes products sold online as “Research Use Only,” such as BPC-157 and TB-500. These are not approved for human use. In fact, when a product says “Not for Human Use,” but the marketing language and buyer behavior clearly suggest otherwise, serious legal and regulatory issues can arise. Regulators do not only look at what the label says. They also look at how the product is marketed, sold, and intended to be used.
For unapproved peptides without systematic human research, we often do not know the appropriate dose, the proper frequency of use, or the long-term safety profile. There is also the very real issue of product quality. Is the product what it claims to be? Is it contaminated? Is it under-dosed, over-dosed, or mixed with something else?
Many users share personal stories online, saying, “I felt great when I used it.” But personal experience is not the same as clinical evidence. It also cannot rule out placebo effects.
Rick’s message was not simply that people should know more peptide names. His bigger point was that the peptide boom is pushing medical, regulatory, and drug-approval issues into the hands of everyday consumers. For professionals, the danger is not just being unfamiliar with a specific peptide. The bigger danger is failing to recognize that different categories of peptides carry very different levels of evidence, legal responsibility, and health risk.
Dr. Seiji Aoyagi: With GLP-1, Eating Less Is Only the Beginning
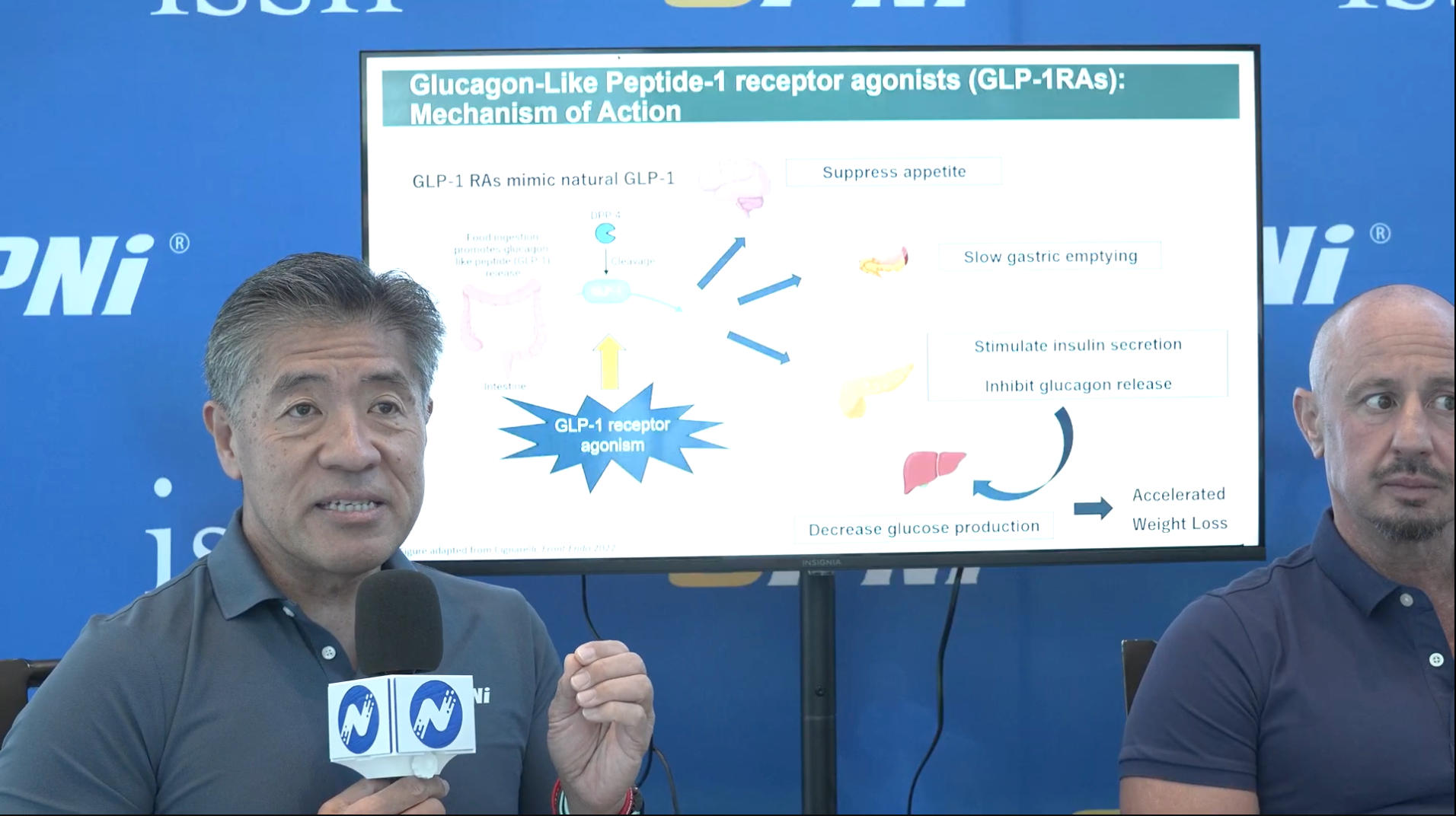
Dr. Seiji Aoyagi, GPNi Japan Director, focused on the nutrition side of GLP-1 use. He began by explaining that GLP-1 itself is a naturally occurring hormone released by the small intestine. What people commonly refer to as GLP-1 drugs are more accurately GLP-1 receptor agonists. These medications can suppress appetite, slow gastric emptying, and influence insulin and glucagon responses. That is why they can help with blood glucose control and weight management.
But Dr. Seiji emphasized that GLP-1 use is not just about eating less and losing weight. If total food intake drops but food quality does not improve, protein intake may fall too low. If resistance training is not included, part of the weight loss may come from lean mass. Many users also experience gastrointestinal side effects, including nausea, vomiting, and diarrhea. These symptoms can further reduce appetite and limit food choices.
Over time, this can affect strength, metabolism, physical function, and body composition. Some individuals may also experience weight regain after stopping treatment, especially if their eating habits and lifestyle have not changed.
Dr. Seiji made an important distinction between weight loss and fat loss. Losing weight simply means the number on the scale goes down. Losing fat while preserving muscle is a very different goal.
He gave a practical example. Many individuals with obesity may already have diets that are relatively low in protein and higher in fat. If GLP-1 use simply reduces the total amount of food they eat, without changing the structure of the diet, protein intake may drop even further. But if the diet is adjusted to be higher in protein and lower in fat, daily protein intake can increase substantially. The difference may be close to 100 grams of protein per day. For someone trying to preserve muscle, improve body composition, or maintain training performance, that gap matters.
Dr. Seiji also mentioned how common these interventions have become in parts of North America. In some walk-in wellness clinics, services related to GLP-1, testosterone, NAD+, and other health optimization programs are now highly visible and easy to access. From the perspective of other markets, that may seem surprising. But even when these services become routine, injections alone do not solve the problem. Nutrition guidance, lifestyle change, and long-term eating habits still matter.
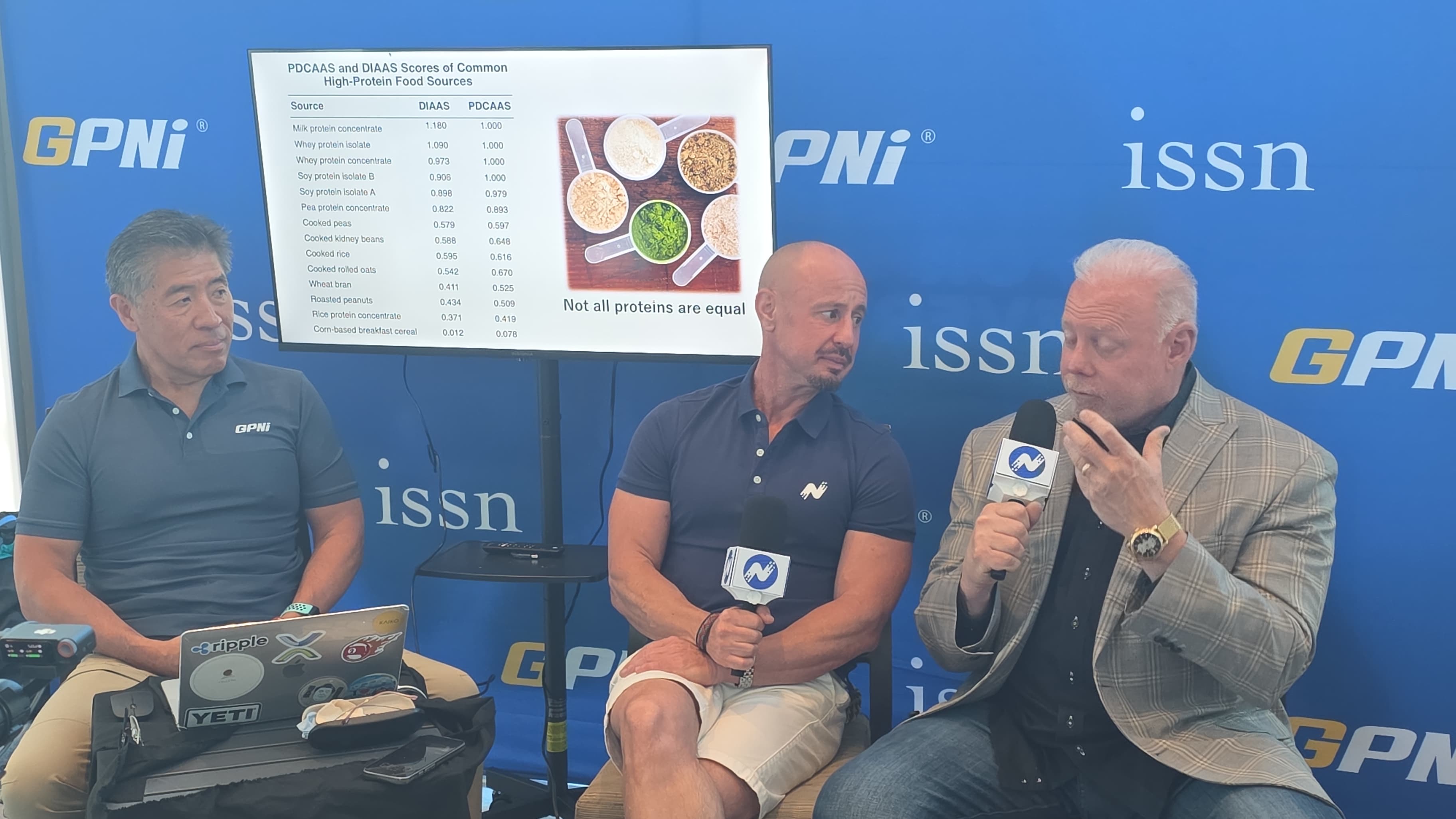
Dr. Seiji also discussed protein quality. He explained that DIAAS focuses on digestible indispensable amino acids and gives a more accurate picture of how well a protein is digested, absorbed, and used by the body. Drew summarized the point in a memorable way: nutrition is not only about what you eat. It is about what you digest, absorb, and assimilate. In other words, protein intake is not just about grams. It is also about digestibility, essential amino acid content, and whether that protein can truly support muscle protein synthesis and recovery.
This matters even more for GLP-1 users. Their appetite is lower. Their gastrointestinal tolerance may change. So the advice cannot stop at “eat more protein.” Professionals need to consider protein quality, format, meal timing, training status, and individual tolerance.
During the Q&A, a participant asked whether very high protein intakes apply to GLP-1 users. Drew clarified that the 3 g/kg figure discussed during the session came from Dr. Jose Antonio’s research in athletic populations. It was not meant as a direct recommendation for GLP-1 users. For this group, the range Dr. Seiji discussed was closer to 1.3–1.6 g/kg.
Dr. Seiji and Drew both emphasized that GLP-1 can help reduce appetite, but it does not replace nutrition planning or training. Rick added another important point: GLP-1 can be a valuable tool, but it is not a magic bullet. Without lifestyle change, high-quality protein, resistance training, and appropriate medical and nutrition supervision, it is easy to mistake weight loss for improved health.
Q&A: Not Just Peptides, but Real Nutrition Questions
After the presentations, the session moved into Q&A. The questions quickly moved from theory into practice.
One participant asked whether Rick could recommend reputable peptide companies. Rick did not name companies. Instead, he reframed the question. The real question is not simply, “Which company is reputable?” The more important question is whether the product exists within a proper framework of legality, evidence, and medical supervision.
In the United States, if a non-food product is intended to affect the structure or function of the body, it may fall under the definition of a drug. So even if a product is labeled “Not for Human Use,” the sales context and intended use still matter. If the product is effectively being marketed for human use, legal and regulatory concerns follow. That point applies beyond the label. We cannot judge these products only by packaging, online testimonials, or user anecdotes. Is the product approved? Does it have human clinical data? Is there medical oversight? Is the sales environment compliant? Those are the questions that matter.
Another question brought the conversation back to a more traditional supplement: creatine.
Participants asked about dosing. For general exercise and maintaining muscle creatine stores, Dr. Seiji and Drew agreed that 3–5 grams per day is a common approach. Drew also noted that creatine is one of the most studied supplements in sports nutrition, and that the ISSN has a comprehensive position stand covering its safety, effectiveness, and dosing. The discussion also touched on creatine and brain health. More people are now looking at creatine beyond muscle and performance, including possible roles in cognition and memory. Some individuals experiment with higher doses. Still, for most people, 3–5 grams per day remains the more common and practical baseline strategy.
Participants also asked about artificial sweeteners, including aspartame. Drew’s response was direct. He is not personally a supporter of aspartame and does not generally recommend it. On sucralose, he was somewhat less concerned, although he noted that some individuals may experience gastrointestinal discomfort or bloating.
The conversation then moved to other sweeteners, including stevia and monk fruit. Dr. Seiji said monk fruit can be a good option, but it is still very sweet. He used that point to make a broader observation: sweetness preference can be trained. If someone regularly consumes very sweet foods and drinks, they become accustomed to that level of sweetness. If they gradually reduce sweetness, their palate can adapt. Drew added that demand for natural sweeteners is rising, but from a formulation standpoint, artificial sweeteners often deliver the familiar sweetness profile consumers expect. Natural sweeteners can be more challenging to work with.
These questions were not all directly about peptides. But that is exactly what made the Q&A useful.
In real practice, sports nutritionists, dietitians, coaches, and health professionals do not receive questions in neat categories. A client may ask about peptides one day, creatine the next, and sweeteners or protein intake after that. The professional challenge is not simply knowing the latest buzzwords. It is knowing how to place those questions within a larger framework of evidence, regulation, training, nutrition, and long-term health.
This GPNi webinar was only the beginning. The full replay and highlight clips are now in production. For those who missed the live session, the replay will offer a more complete way to follow the discussion. For those who attended live, watching it again may help reinforce the key points around regulation, nutrition, and practical decision-making.
GPNi will continue to host discussions around sports nutrition and emerging topics in health and performance. The trends will keep changing. Professional judgment will only become more important.